Stay Informed
Follow us on social media accounts to stay up to date with REHVA actualities






Ten percent
of Europeans report having poor perceived general health. And the probability
that a person reports poor health increase up to 70% if that person also lives
in an unhealthy building vs. a healthy one. The results of this study show a
correlation between poor health and the specific unhealthy building factors:
·
1.7
times report poor health in a damp building
·
1.5
times report poor health when living in a building with insufficient daylight
·
1.3
times report poor health when perceiving overheating
·
1.7
times report poor health when living in uncomfortably cold temperatures
The paper
is based on the analysis of the correlation between health and buildings in 27
EU member states using the Eurostat database EU-SILC (Survey on Income and
Living Conditions). The presented research is based on EU-SILC raw data. For
the purpose of the study, Eurostat approved the research proposal behind the
analysis and gave access to the data to Ecofys
Germany GmbH.
Around 508 million European citizens (EUROSTAT, 2015) spend about 90% of their time indoors (living and working) (NEST, 2004). Therefore Europe‘s buildings have a major impact on Europeans‘ health. According to WHO‘s definition (since 1948) “Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”
Yet, research assessing the statistical links between health and housing conditions is largely missing. Considering that building renovation is a huge intervention into the whole building system – cross-cutting technical aspects of the building itself and social as well as economic issues of the dwellers – it is necessary to fully grasp the implications, risks and chances. Therefore, a main research objective is to identify these links and to highlight which part of Europe's and MS’s population is most in need of building renovation.
This insight triggered a detailed study on the relation between health and housing conditions across EU28 and its Member States. The results described here have been presented in the scientific report “The relation between quality of dwelling, socio-economic status and health in EU28 and its Member States” (Hermelink & John, 2017).
This
article is based on a paper presented at the 38th AIVC - 6th TightVent &
4th venticool Conference, 2017 “Ventilating healthy low-energy buildings” held
on 13-14 September 2017 in Nottingham, UK.
The results
from the study are used in VELUX Healthy Homes Barometer 2017.
The research is based on analysing Eurostat microdata from the EU-wide survey „Income and Living Conditions in Europe“ (EU-SILC). EU-SILC is a Eurostat Survey, which is conducted in a European-wide household panel, to assess the status and development of Income and Living Conditions in Europe. The EU SILC survey covers amongst others the domains housing including economic issues and health. Data in EU-SILC are collected either on household or individual level. For this research, anonymised results for more than 100,000 individual households and more than 250,000 adults (16 +) across all EU Member States – except Germany - were made available by Eurostat. The focus of this study lies on data from 2012, where more detailed information on housing conditions was collected. To handle the massive amount of data the statistical computing program R (version 3.3.0) was used for statistical analyses of the microdata.
The research reveals that around 16% of Europeans report deficiencies regarding the building status; either because of dampness (leaking roof or damp floor, walls or foundation), lack of daylight, inadequate heating during the winter or overheating problems. The analysis also shows that around 44 Mio adults report poor perceived general health; this is equivalent to nearly 10% of the European population. As described above, the results will focus on the linkage between building status and health. Accordingly, the focal point of analysis described here are:
· health in damp buildings,
· health in dark buildings,
· health in overheated buildings,
· health in building with uncomfortably cold temperatures.
Detailed results of each of the mentioned topics will be described in the following subsections.
15% of EU households (more than 30 Mio; or more than 60 Mio adults) report to live in damp buildings (leaking roof, damp floor/walls /roof/ foundation etc.).
· When adults report no dampness 9% report poor health.
· When adults report dampness 16% report poor health.
The
probability that adults report poor health is significantly higher in homes
with reported dampness; across the EU the probability is 1.7 times higher than
with no dampness.
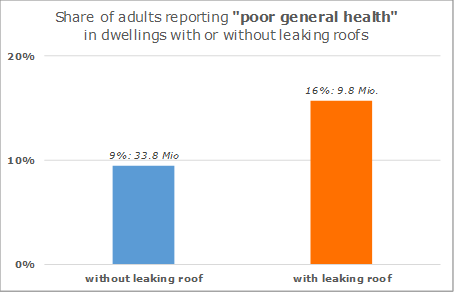
Figure 1. Health status in damp buildings for EU28 (share within subset and number of adults).
Approx. 6% of all EU households (14 million; or approx. 30 Mio adults) report a lack of daylight
· When adults report no lack of daylight 10% report poor health.
· When adults report lack of daylight 15% report poor health.
The probability that adults report bad health
is significantly higher when a lack of daylight is perceived; across the EU
this probability is 1.5 times
the one when no lack of daylight is perceived. Altogether approx. 10% of all adults reporting poor health live in
buildings lacking daylight, where only 7% of all adults live.
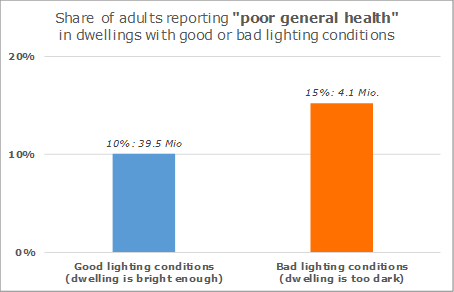
Figure 2. Health status in dark building for EU28 (share within subset and number of adults).
Approx. 20% of all EU households (40 million; or approx. 84 Mio adults) report bad thermal comfort in summer.
· When adults report good thermal comfort (cool dwelling) in summer, 10% report poor health.
· When adults report bad thermal comfort (too hot dwellings) in summer, 13% report poor health.
The probability that adults report bad health is significantly higher when the bad thermal comfort is perceived; across the EU this probability is 1.3 times when good thermal comfort is perceived.
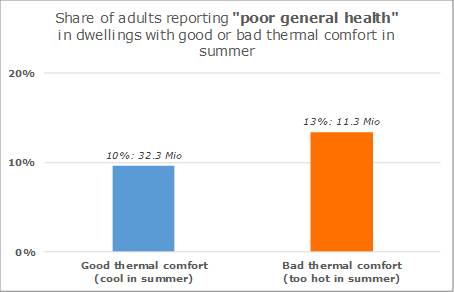
Figure 3. Health in overheated buildings for EU28 status (share within subset and number of adults).
Approx. 15% of all EU households (more than 30 Mio; or more than 60 Mio adults) bad thermal comfort in winter
· When adults report good thermal comfort (warm dwellings) in winter 9% report poor health.
· When adults report bad thermal comfort (too cold dwellings) in winter 16% report poor health.
The probability that adults report bad health is significantly higher when bad thermal comfort is perceived; across the EU this probability is 1.7 times the one when good thermal comfort is perceived.
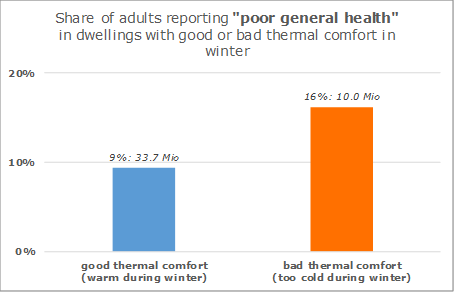
Figure 4. Health in too cold buildings for EU28 status (share within subset and number of adults).
The results described in this paper based on EU-SILC variables on quality of buildings and general health show statistically significant interdependencies. However, additional analysis are needed to understand for example the influence of economic issues of households and individuals, regional patterns or energy poverty on health. Based on the results shown here, we observed that structural problems of the building like leaking roofs, damp walls (etc.), buildings’ ability to provide comfortable temperatures in winter, lack of daylight seem to act as similarly strong accelerators and/or indicators for health problems. On average the relative share of adults reporting poor health increases 30 to 70% when at least one of the above-mentioned deficiencies is reported compared to the group of people who do not perceive such deficiencies.
However, as
indicated above this study so far focused on a small selected sample of
relevant variables influencing health. On the other hand
like in the analyses of Thomson
and Snell (2012) who focused their EU SILC analyses on energy poverty, the
strengths of the correlations are moderate. This is why on the one hand we
found statistically highly significant correlations between the presented
variables. This means, that there are many other variables apart from the ones
analyzed in this study, also having a very significant impact on a person’s
perceived general health. Obviously personal and environmental variables
determine health. Yet, we feel that buildings, which in this equation at least
in Europe occupy 90% of the environmental variables’ time are very much
under-represented in today’s overarching discussion about sustainability, which
eventually is about shaping the world in a way that leads to sustained
individual and societal health.
Above mentioned problems like dampness, darkness, too cold in winter or overheating in summer clearly hint at buildings in need of renovation. According to EUROSTAT (2012), ca. 58% of EU’s population live in detached and semi-detached single-family homes; our results also show that around 4 out of 5 of these dwelling types are owned by private owners. This means, that this group is crucial to successfully increase the renovation rate as implicated in the proposal for the amending directive on energy performance of buildings (European Commission, 2016) and needs to be addressed by incentives, renovation policies and awareness raising as well as information campaigns.
To reveal more insights, further research is ongoing to examine the linkage between health and building status, but also considering the economic status of building’s occupants. This analysis considers additional variables such as health prevalence of building occupants for example due to age, occupancy status and, economic status, income level, existing chronical illnesses, medical care system of respective country, etc. In this sense, a prediction model and additional multiple correlations for health considering selected variables of building and economic status and previous mentioned variablescould reveal insights on the impact on health, but also more general insights into causes and effects within the triangle of clusters of variables described above. Furthermore, analysis shall evaluate the development of the building and economic status as well as general health aspects over time to observe the impact of policy measures and to derive recommendations for priority areas for action. This can also reveal insights on causal chains between building status, economic situation and health aspects explaining energy poverty.
This research was supported by VELUX A/S. The research was conducted by experts from Ecofys Germany GmbH, with assistance of experts from VELUX A/S.
EUROSTAT (2012): Description of Target Variables: Cross-sectional and longitudinal. 2012 operation (Version May 2013). Ed. European Commission. Brussels.
EUROSTAT (2012). Distribution of population by dwelling type. (online data code: ilc_lvho01), accessed 04.06.2017.
European Commission (2016). Proposal for a Directive of the European Parliament and of the Council amending Directive 2010/31/EU on the energy performance of buildings.
EUROSTAT (2015). Population on 1 January by age and sex. (online data code: demo_pjan). accessed 04.06.2017.
European Commission (2017): EU Building Stock Observatory. Online: https://ec.europa.eu/energy/en/eubuildings, accessed 01.06.2017.
Gruen, G. and Urlaub, S. (2014): White Paper: Towards an Identification of Europeanindoor environment’ impact on health and performance – homes and schools. Fraunhofer IBP. Holzkirchen. Online: https://www.ibp.fraunhofer.de/content/dam/ibp/de/documents/Presseinformationen/Velux-Prestudy_WhitePaper_141205_amended.pdf, accessed 04.06.2017.
Hermelink, A. and John, A. (2017). The relation between quality of dwelling, socio-economic status and health in EU28 and its Member States. Scientific report as input for Healthy Home Barometer 2017. Cologne. Ecofys by order of VELUX A/S. Online: http://www.ecofys.com/files/files/ecofys-2017-relation-between-quality-of-dwelling-and-health-final.pdf, accessed 01.06.2017.
NEST (2004): NEST project, Technical University of Berlin, European Commission 2004. quoted from Velux (2015). Healthy Home Barometer 2015.
Thomson, H. and Snell, C. (2012). Quantifying the prevalence of fuel poverty across European Union. Energy Policy, 52 (2013), 563-572
Velux (2015): Healthy Homes Barometer 2015. Online: http://www.velux.dk/~/media/marketing/master/documents/pdf/brochures/velux_hhb_18032015.pdf, accessed 01.06.2017.
Velux (2016): Healthy Homes Barometer 2016. Online: http://www.velux.com/article/2016/europeans-on-healthy-living-the-healthy-homes-barometer-2016, accessed 01.06.2017.
Velux (2017): Healthy Homes Barometer 2017. Online: http://velcdn.azureedge.net/~/media/com/health/healthy-home-barometer/507505-01%20barometer_2017.pdf, accessed 01.06.2017.
WHO (1946): Constitution of the World Health Organization. Online: http://apps.who.int/gb/bd/PDF/bd47/EN/constitution-en.pdf?ua=1, accessed 04.06.2017.
Follow us on social media accounts to stay up to date with REHVA actualities
0