







Stay Informed
Follow us on social media accounts to stay up to date with REHVA actualities
|
|
|
|
Arsen K. Melikov | Angui Li | Risto Kosonen | Xianting Li |
International Centre for Indoor Environment and Energy, Department of Civil Engineering, Technical University of Denmark, Denmarkakm@byg.dtu.dk | School of Building Services Science and Engineering, Xi’an University of Architecture and Technology, Xi’an, China | Department of Mechanical Engineering, School of Engineering, Aalto University, Espoo, Finland | Beijing Key Laboratory of Indoor Air Quality Evaluation and Control, Department of Building Science, School of Architecture, Tsinghua University, Beijing, China |
|
|
|
|
Zhang Lin | Guangyu Cao | Bin Yang | |
Division of Building Science and Technology, City University of Hong Kong, China | Department of Energy and Process, Norwegian University of Science and Technology, Trondheim, Norway | School of Building Services Science and Engineering, Xi’an University of Architecture and Technology, Xi’an, China |
At present total volume air distribution (TVAD), primarily mixing ventilation, is most commonly applied in practice. This ventilation is also known as ventilation by dilution. The goal is to mix as completely as possible the supplied clean air with the polluted and most often warm room air and to obtain uniform temperature, humidity and contaminant distribution in the occupied zone of rooms. However, the strategy of TVAD is inefficient. Clean and cool air is supplied far from occupants, typically from diffusers located on the ceiling and is mixed with room air. The supply air becomes warm and polluted and possibly contains infectious agents exhaled by respiration activities of sick people before it reaches the occupants. The air distribution pattern of mixing ventilation enhances the transport of pollution generated outside of the occupied zone (e.g., from wall surfaces, etc.) into the occupied zone (Figure 1). Complex interactions of supplied ventilation flow, thermal plumes from occupants and buoyancy flows from cold/warm objects and surfaces (walls, windows) determine temperature, velocity and contaminant distribution in spaces. These interactions have a large impact on indoor air quality. However, it is difficult to control the interactions because they depend on the strength and changes in time of the heat loads distribution, the characteristics of the supplied air jets in their fully developed region (which are not easy to control), etc.
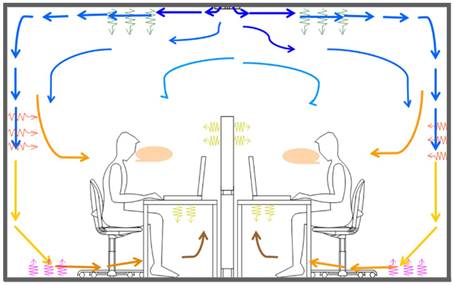
Figure 1. Mixing ventilation. Pollution generated by building materials and office equipment is mixed with the supplied clean air, transported to occupied zone and inhaled by occupants.
Design aimed at a uniform temperature and velocity in the occupied zone does not respond to the large differences between occupants with regard to the preferred environment. Therefore, occupants report often dissatisfaction with the indoor air quality and thermal conditions, though the recommendation prescribed in the indoor climate standards are met. The supply of large amounts of clean and cool air are needed to maintain temperature and pollution concentration at acceptable levels in the entire space (including unoccupied areas) leading to increased energy consumption and use of large and costly air handling and ducting systems. Flexibility in space use, which is an important requirement in many office buildings, hospitals, etc., is curtailed. Once installed, air supply devices can be difficult to reposition (except for some floor diffusers) in order to generate proper air distribution after the furniture layout is changed.
The stated above disadvantages of mixing ventilation call for the need to develop new ventilation methods able to provide a better indoor environment for occupants at reduced energy consumption. At the same time, the methods should provide efficient and smart control and flexibility in space use. Occupant targeted ventilation has the potential to fulfil these requirements.
Occupant targeted ventilation (OTV) is based on the occupant centred principle with advanced clean air distribution [1]. The existing practice of air conditioning and air transportation is applied during the design. The OTV focuses on two important elements – health and comfort for individual and group occupants and non-uniform air distribution. Efficient control of the air distribution is an important advantage of targeted ventilation. OTV can be implemented in different spaces in hospital facilities, public buildings, shops, schools, etc. Two examples of OTV, namely localized chilled beam [2] and wall-attached ventilation [3] are shown in Figure 2. The performance of other designs and applications of OTV have been studied and reported in the literature: stratum ventilation [4], protected zone ventilation [5], personalized ventilation [6], localized combined radiant and convective microenvironment systems [7], etc.
Occupant targeted ventilation is the next, natural step in the development of room air distribution practice in occupied spaces after total volume ventilation (mixing and displacement). OTV is based on efficient methods and devices for air distribution to the target area, i.e. as close as possible to the breathing zone of single or group of occupants. Therefore, occupants breathe cleaner air compared to total volume ventilation. OTV has higher potential for reduction of the risk of airborne cross-infection compared to the total volume ventilation as well.
An important advantage of OTV is that its design considers the activities of each occupant or group of occupants, supply air demands, adjustability, functionality and flexibility according to the needs that may change in time and space. As already noted, some OTV methods are known and already used in practice; others are newly developed. Some OTVs utilize the existing design and implementation of air transportation to the spaces as used today for mixing and displacement ventilation. Therefore, its design and implementation in practice is easy for consultants.
Occupant targeted ventilation has the potential to perform better than total volume ventilation with regard to energy consumption. OTV is designed to focus on the changing in time needs and activities of each occupant or group of occupants. Therefore, the ventilation air can be supplied when, where and as much as needed. This principle may lead to a reduction in energy consumption.
Occupant target ventilation is occupant-centred. This allows more sophisticated and efficient control, including smart and intelligent control, compared to the control strategies for mixing ventilation. These control strategies make it possible to improve the micro-environment (inhaled air quality and thermal comfort) for each occupant (e.g., the localized chilled beam shown in Figure 2) and a group of occupants as well as to reduce energy use. Intelligent sensing of occupants’ body physiological signals and positioning are used as feedback signals to control target ventilation[8, 9].
Several solutions of OTV have already been implemented and performed successfully in practice. The coming soon new REHVA guidebook on Occupant Targeted Ventilation will present new solutions together with numerous case studies to help consultants and designers for the OTV to prevail in practice.
|
|
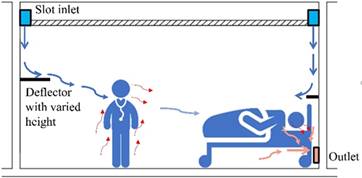
Figure 2. Examples of OTV: left - localized child beam with direction and strength of the supplied flow rate under the control of the occupant [2], right - wall attached ventilation providing clean air to the breathing zone of the two occupants and removing locally the air exhaled by the patient [3]. | |
Considering the importance of COVID 19 pandemic at present, in the following, the performance of OTV for the reduction of the airborne cross-infection between occupants in an office room (length 10 m × width 5 m × height 2.7 m; 50 m³) with 10 occupants (one infected occupant and nine susceptible occupants) is presented as an example. The room is ventilated by a supply of 118 ℓ/s (423 m³/h) outdoor air, i.e., 2.35 ℓ/s m³ (8.46 m³/h m³). The supplied air aims removal of pollution generated by occupants and pollution generated from building materials: 100 ℓ/s (360 m³/h) corresponding to 2 ℓ/s m³ (7.2 m³/h m³) is supplied for removal of pollution generated by occupants, i.e., 10 ℓ/s per person, and additional 18 ℓ/s (63 m³/h), corresponding to 0.35 ℓ/s m³ (1.26 m³/h m³), for removal of pollution generated by building materials (very low polluting buildings, category II – EN16798 [10]).
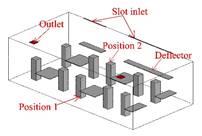
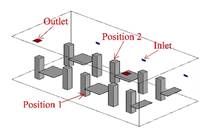
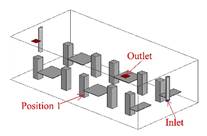
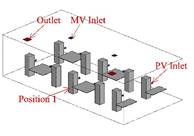
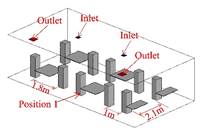
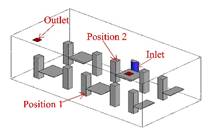
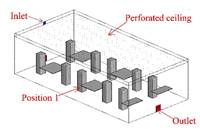
Four OTV methods, namely wall attached ventilation (WAV), stratum ventilation (SV), personalized ventilation (PV) and impinging jet ventilation (IJV), are considered (Figure 3). The methods employ non-uniform occupant-centred distribution of clean air supplied to spaces. In addition, the used at present mixing (MV), displacement ventilation (DV) and diffuse ceiling ventilation (DCV) are considered as well for the purpose of comparison. The geometry of the room, the layout of the ten workstations and the size and location of supply and exhaust diffusers are presented in detail in [11]. The layout in the simulated room, location of air supply and exhaust terminals and the simulated two positions (1 and 2) of the infected occupant are shown in Figure 4.
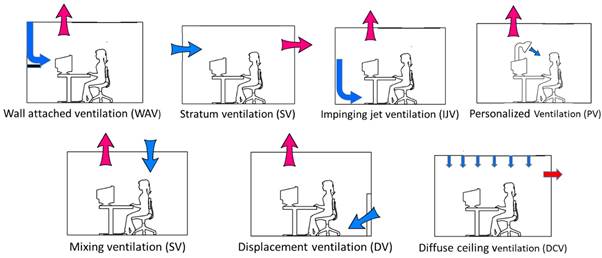
Figure 3. The simulated air distribution methods (blue arrows: supply; red arrows: exhaust).
The Computational Fluid Dynamics (CFD) method, validated with full scale physical measurements, was used to simulate the office, the occupants and the studied air distribution methods. Based on the CFD simulations, the exposure of the susceptible occupants to the infected air exhaled by the sick occupant was calculated. The probability of infection was calculated using the modified Wells-Riley model considering the non-uniformity in the spread of the infectious exhaled air. The details of the applied method are provided in [11].
The simulation results related to the risk of airborne transmission are shown in Figure 5. The infection probability for the studied cases, including the two locations of the infected occupant, P1 and P1, for the WAV, SV and DV and one location, P1 (assuming symmetry in the room air distribution) for the IJV, MV, PV and DCV is compared. The median, the 25 and 75 percentiles, and the 5 and 95 percentiles are shown in the figure. The red dotted line indicates the infection risk predicted with the original Wells-Riley model when assuming perfect mixing of the supplied air with the room air [12].
|
|
a) Wall attached ventilation (WAV). Slot inlets 1&2: 1.8 m × 0.02 m & 3.6 m × 0.02 m (L × W) Deflector 1: 1.8 m × 0.4 m (L × W), 1.2 m above floor Deflector 2: 3.6 m × 0.4 m (L × W), 1.2 m above floor | b) Stratum ventilation (SV). Three inlets: 0.30 m × 0.10 m (L × W), 1.3 m above floor |
|
|
c) Impinging jet ventilation (IJV). Semi-circular inlet: radius 0.15 m, 0.95 m above floor | d) Personalized ventilation (PV) combined with MV. MV inlet: 0.25 m × 0.25 m (L × W), PV inlet: radius: 0.06 m; 0.30 m (in front of the face of each occupant) |
|
|
e) Mixing ventilation (MV). Ceiling inlet 0.25 m × 0.25 m (L × W) | f) Displacement ventilation (DV). Semi-circular inlet - radius 0.25 m, height 0.97 m |
| |
g) Diffuse ceiling ventilation (DCV) with perforated ceiling. | |
Figure 4. The simulated office room. Air supply and exhaust diffusers indicated respectively as “inlet” and “outlet”. Outlet size in all cases: 0.2 m × 0.2 m (L × W) | |
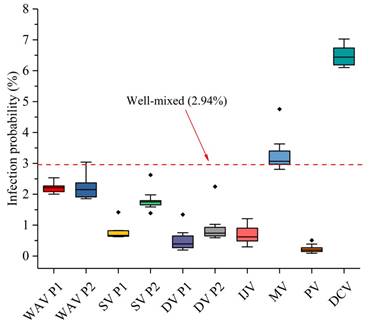
Figure 5. Infection probability at the faces of nine susceptible persons under ten simulation cases (maximum, minimum, quarter, three-quarter and median values are shown).
The results in Figure 5 show the potential of OTV methods for achieving lower infection probability compared to mixing ventilation (MV) and diffuse ceiling (DCV).
REHVA Guidebook on design of Occupant Targeted Ventilation is under preparation. The guideline will include design procedure and recommendations as well as cases of design and implementation of OTV in practice.
[1] Melikov, A., 2011, Advanced air distribution, ASHRAE Journal, November 2011, pp. 73-78.
[2] Arghand T., Melikov A.K., Bolashikov Z., Kosonen R., Aho I., et al. 2016. Individually controlled localized chilled beam in conjunction with chilled ceiling: Part 2 – Human response, Proceedings of the 14th International Conference on Indoor Air Quality and Climate, Ghent, Belgium, July 3 – 8 2016, Paper ID: 482.
[3] Li A. Extended Coanda Effect and attachment ventilation, Indoor and Built Environment, 2019, Vol. 28(4) 437–442.
[4] Lin, Z., Yao, T., Chow, T.T., Fong, K.F., Chan, L.S., 2011, Performance Evaluation and Design Guidelines for Stratum Ventilation. Building and Environment, 46: 2267-2279, https://doi.org/10.1016/j.buildenv.2011.05.006.
[5] G. Cao, P. V. Nielsen, R. L. Jensen, P. Heiselberg, L. Liu, J. Heikkinen, 2015, Protected zone ventilation and reduced personal exposure to airborne cross‐infection, Indoor Air, 25, 3, 307-319, https://doi.org/10.1111/ina.12142.
[6] Melikov, A.K., 2004, Personalized ventilation, Indoor Air, vol. 14, supplement 7, pp. 157-167.
[7] Zhao W, Kilpeläinen S, Kosonen R and Jokisalo J. Experimental comparison of local low velocity unit combined with radiant panel and diffuser ceiling ventilation system. Indoor and Built Environment. Special-Issue RoomVent 2018 (accepted 21.3.2020). https://doi.org/10.1177/1420326X20918398.
[8] Yang, B., Li, X., Hou, Y., Meier, A., Cheng, X., Choi J-H, Wang, F., Wang, H., Wagner, A., Yan, D., Li, A., Olofsson, T., Li, H. 2020. Non-invasive (non-contact) measurements of human thermal physiology signals and thermal comfort/discomfort poses-A review. Energy and Buildings, 224, 110261.
[9] Li, X., Liu, Y., Liu, P., Ren, Q., Li, A., Yang, B., Cheng, X., Chen, J. 2021. Application of computer vision technologies in collecting HVAC control signals. HV&AC (Chinese Journal), 51(6), 1-12.
[10] European standard EN 16798-1:2019. Energy performance of buildings – Ventilation for buildings – Part 1: Indoor environmental input parameters for design and assessment of energy performance of buildings addressing indoor air quality thermal environment, lighting and acoustics – Module M1-6, May 2019, European Committee for standardization, Brussels.
[11] Su W. et al. Infection probability under different air distribution patterns, Building and Environment Volume 207, Part B, January 2022, 108555.
[12] Riley E C, Murphy G, Riley R L. Airborne spread of measles in a suburban elementary school. American Journal of Epidemiology, 1978, 107(5): 421-432.
Follow us on social media accounts to stay up to date with REHVA actualities
0