

Stay Informed
Follow us on social media accounts to stay up to date with REHVA actualities
This article is based on a paper presented at the 42nd AIVC - 10th TightVent & 8th Venticool Conference “Ventilation Challenges in a Changing World” held on 5-6 October 2022 in Rotterdam
|
|
Andrew Persily | Oluwatobi Oke |
National Institute of Standards and TechnologyGaithersburg, Maryland 20899 USA | National Institute of Standards and TechnologyGaithersburg, Maryland 20899 USA |
The COVID-19 pandemic highlighted the importance of ventilation in mitigating the spread of airborne infectious diseases. As a result, many organizations have made recommendations for improved ventilation [1-2]. These include increased ventilation rates, higher efficiency filtration, and portable air cleaners. Real-time monitoring of indoor CO₂ concentrations is also recommended as an indicator of ventilation adequacy [3-5]. However, guidelines for CO₂ monitoring vary, and their technical bases are not fully described in all these recommendations. In addition, CO₂ has been used in modeling and experimental studies motivated by the pandemic.
The relationship of indoor CO₂ to ventilation and indoor air quality (IAQ) has a long history, dating back centuries. These discussions have evolved to include 1) the relationship between CO₂ and bioeffluent odors, 2) the impacts of CO₂ on building occupants, 3) the use of CO₂ as a tracer gas to measure air change rates and ventilation performance, and 4) outdoor air intake control using CO₂ concentrations. Recently, CO₂ has also been discussed in response to the pandemic in relation to the risks of airborne disease transmission. The ASHRAE Position Document on Indoor Carbon Dioxide [5] describes the relationship of CO₂ to ventilation and IAQ, documenting the solid knowledge base that exists to support the application of CO₂ monitoring and analysis. This article summarizes how CO₂ monitoring and simulation have been applied in response to the COVID-19 pandemic. Only limited references are provided, with a more complete list available in reference 6. The authors are pursuing a more comprehensive scoping review that will be published later this year.
In response to COVID-19, there have been several research studies and guidance documents describing the use of indoor CO₂, which are all based on established concepts. However, the technical basis for the applications, recommendations, and supporting documents is not always clear. This review considered these applications, including tracer gas measurements of air change rates and ventilation performance, CO₂ as an indicator or proxy of infection risk, indoor CO₂ concentrations as indicators of ventilation or IAQ, and recommendations on the use of CO₂ monitoring.
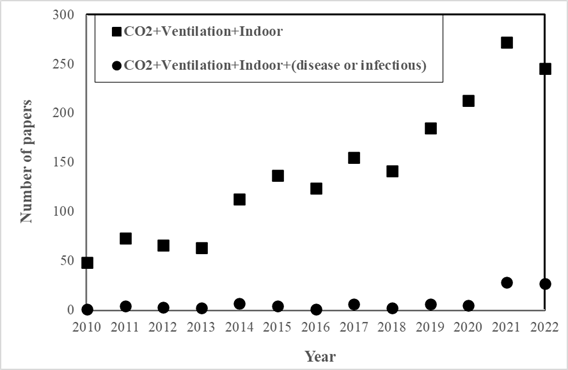
Figure 1. Number of papers related to indoor CO₂ as a function of year (as of 23 Feb 2023).
As an indication of increased interest in CO₂, Figure 1plots the number of papers published by year, based on Web of Science searches, using the terms “carbon dioxide ventilation building” and the same terms with the addition of “disease” OR “infectious”. The number of papers related to CO₂ and ventilation in buildings has been increasing since 2014, with another increase in 2021, presumably due to the COVID-19 pandemic. The number of papers that mention “disease” OR “infectious” increased even more dramatically in 2021.
Many field studies have measured air change rates using standard single-zone tracer gas decay or constant injection, with the latter assuming steady-state CO₂ concentration. These measurements have been conducted in various settings, such as schools, gyms, buses, and retail buildings, to evaluate transmission risk or IAQ. In addition, some measurements have been done using transient or integral mass balance analyses that are not standardized. Some studies have been conducted in naturally ventilated spaces, but applying tracer dilution methods to these spaces can be challenging due to the difficulty in achieving uniform tracer gas concentrations. A few studies used CO₂ as a tracer gas to measure air change rates in laboratory chambers for air cleaner performance testing. These environments are well-controlled, making measurements easier and the results more likely to be valid.
However, these studies involving air change rate estimation vary in their discussion of key assumptions and inputs. For example, some studies lack detail on the CO₂ generation rate, which varies based on occupancy. In addition, some use measured outdoor CO₂ concentrations, while others use an assumed value, which may not be reliable given variations in outdoor concentrations. Another critical assumption is that these tracer gas methods assume the space being studied behaves as a single zone, but most studies do not mention or justify this assumption. Finally, measurement uncertainty is not usually reported, making it difficult to interpret results.
Several studies have used CO₂ as an indicator or proxy for exposure to infectious aerosols or infectious risk through measurements in the field of test chambers and simulations using computational fluid dynamics (CFD). Experimental studies have been conducted in various space types, including concert halls, healthcare facilities, and laboratory chambers. Some studies simultaneously measured CO₂ and airborne particle concentrations to study their relationship, while others used CO₂ concentration as an indicator of exposure or risk using the Wells-Riley equation. Others present CO₂ as a risk indicator without explaining the basis for the connection. Many studies employ the concept of rebreathed air, and some focus on the impact of specific activities like breathing, talking, or signing or features such as ventilation rates, physical partition, and filtration.
Several modeling studies have used CO₂ as an indicator of aerosol exposure and infection risk, using CFD to examine the impact of air distribution. Others used mass balance modeling to evaluate CO₂ variations in space and time as exposure or risk indicators, sometimes acknowledging that there is no direct evidence correlating CO₂ concentrations with virus-containing aerosol levels.
While CO₂ has been used as a surrogate for infectious aerosols, arguments exist for and against. Some reasons for using CO₂ as a surrogate include the ability to capture the fate and transport of fine droplets and simplicity. Reasons against include differences in particle dynamics from gases, two-phase airflow of infectious aerosols, and the inability to capture differences between particles with aerodynamic diameters relevant to virus transmission.
Many field studies of infection risk or building performance during the pandemic have included measurements of CO₂ concentrations, generally as metrics of ventilation and IAQ. However, the links between CO₂, ventilation, and IAQ are not always explained. In many cases, ASHRAE Standard 62.1 [8] is cited as the source of concentration limits of 1000 ppmv or 700 ppmv above outdoors, despite the standard not containing either value. Other studies cite CO₂ limits in documents associated with the country where the measurements were conducted.
These studies include a survey of the indoor environments in taxis in Paris before and after the lockdown and an examination of the effectiveness of ventilation in buses in Spain. Other studies present assessments of ventilation and IAQ in a fitness club, a concert hall, and some mechanically ventilated buildings. Many of these studies simply report the measured CO₂ concentrations, sometimes compared to a local limit, but generally do not discuss the value of CO₂ as a ventilation or IAQ metric. As discussed in [6], indoor CO₂ concentrations are not good indicators of overall IAQ but can serve as a measure of ventilation using tracer gas concepts as discussed above.
Several studies using CO₂ measurement or analysis have been conducted to investigate strategies for monitoring or controlling building ventilation. While these studies generally do not quantify infection risk, they are motivated by the need to manage risk. For example, one proposed feedback control strategy uses CO₂ monitoring as a function of scheduled airing periods, class duration, and masking to manage infection risk in naturally ventilated classrooms. Another used metabolism-based ventilation control to reduce infection risk and energy use in gymnasiums. Others reviewed CO₂ monitoring and ventilation recommendations, noting the challenges in linking CO₂ concentration to infection rates and identifying concentration limits for different spaces.
As noted in the ASHRAE Indoor CO₂ Position Document [6], there are numerous recommendations, and in some cases requirements, to monitor indoor CO₂ concentrations to manage the risks of airborne infection, often with a reference concentration for comparison or compliance. These concentrations are based on CO₂ as an indicator of ventilation or as a direct or indirect indicator of infection risk, but the rationales presented are not always clear.
Indoor CO₂ limits have been established for decades for managing generic IAQ and sick building syndrome symptoms, usually around 1,000 to 1,500 ppmv. During the pandemic, several organizations, and governments have recommended monitoring indoor CO₂ concentrations as an indicator of outdoor ventilation rates [2-4]. However, measured CO₂ concentrations are not considered reliable proxies for the risk of airborne exposure to the SARS-CoV-2 virus [9].
Many of these indoor CO₂ limits are based on CO₂as an indicator of the outdoor ventilation rates, which implicitly involves using CO₂as a tracer gas requires a target ventilation rate. However, the bases for these limits are not always explained. CO₂ limits based can be estimated using the requirements of ventilation standards, e.g., CEN 16798 [10] or some other ventilation rate intended to control transmission. The CO₂ limits that have been issued generally do not differentiate between space types, occupant characteristics, or required ventilation rates, despite their impact on indoor concentrations. A space-specific CO₂ metric for ventilation has been developed that considers the space, occupants, and target ventilation rate [11], which can be applied using an online tool called QICO₂ [12].
This article summarized the application of indoor CO₂ in response to the COVID-19 pandemic. CO₂ has been used as a tracer gas to estimate air change rates and as an indicator of ventilation or IAQ, which are not new concepts. Some studies have focused on CO₂ as a proxy for airborne infectious aerosols. However, these applications do not always reflect a complete understanding of the relevant mass balance theory, building ventilation, and IAQ. The studies reviewed in this summary reinforce the need for better guidance on the use of indoor CO₂, including measurement protocols and research on CO₂ emissions by building occupants, indoor CO₂ concentrations, and the relationship between indoor CO₂ and airborne disease transmission.
[1] ASHRAE. (2022). ASHRAE Building Readiness Guide. American Society of Heating, Refrigerating and Air-Conditioning Engineers. https://www.ashrae.org/file%20library/technical%20resources/covid-19/ashrae-building-readiness.pdf
[2] REHVA. (2021) REHVA COVID19 Guidance. Version 4.1. Federation of European Heating, Ventilation and Air Conditioning Associations.
[3] CDC. (2021). Ventilation in Buildings. Centers for Disease Control and Prevention.
[4] EMG-SPI-B. (2021). Application of CO₂ monitoring as an approach to managing ventilation to mitigate SARS-CoV-2 transmission. UK Scientific Advisory Group of Emergencies, Environmental Modelling Group and Scientific Pandemic Insights Group on Behaviours.
[5] EPA. (2022). Clean Air in Buildings Challenge. U.S. Environmental Protection Agency. https://www.epa.gov/indoor-air-quality-iaq/clean-air-buildings-challenge
[6] ASHRAE (2022). Position Document on Indoor Carbon Dioxide. American Society of Heating, Refrigerating and Air-Conditioning Engineers.
[7] Persily, A. and O. Oke (2022). Application of Indoor Carbon Dioxide During the COVID-19 Pandemic. 42nd AIVC Conference. Rotterdam, The Netherlands: 700-709.
[8] ASHRAE (2022). ANSI/ASHRAE Standard 62.1-2022, Ventilation for Acceptable Indoor Air Quality, American Society of Heating, Refrigerating and Air-Conditioning Engineers.
[9] AIVC. 2020. Can a measured CO₂ concentration show a building is SARS‐CoV‐2 safe? AIVC Newsletter, November issue, Air Infiltration and Ventilation Centre.
[10] CEN (2019). EN 16798-1:2019, Energy performance of buildings - Ventilation for buildings - Part 1: Indoor environmental input parameters for design and assessment of energy performance of buildings addressing indoor air quality, thermal environment, lighting and acoustics. Brussels, European Committee for Standardization.
[11] Persily, A. (2022). Development and Application of an Indoor Carbon Dioxide Metric. Indoor Air, 32(7), e13059.
[12] Persily, A. and B. J. Polidoro. (2022). Indoor Carbon Dioxide Metric Analysis Tool. NIST Technical Note 2213. National Institute of Standards and Technology.
Follow us on social media accounts to stay up to date with REHVA actualities
0