




Stay Informed
Follow us on social media accounts to stay up to date with REHVA actualities
|
|
|
Nabaneeta SharmaNTNU, Trondheim, Norwaynabanees@stud.ntnu.no | Yang BiNTNU, Trondheim, Norway | Evangelia GiotiNTNU, Trondheim, Norway |
|
|
|
|
|
|
Emma Dyvesveen MyrbekkNTNU, Trondheim, Norway | Guangyu CaoNTNU, Trondheim, Norway |
|
Since 2019, the COVID-19 pandemic has changed the way people lived. Norway imposed restrictions that are divided into three levels of actions, depending on the infection situation: general level (yellow), somewhat elevated level (orange), and more elevated level (red) [1]. These measures include a section dedicated to smaller, closed rooms with group activities at fitness centres, which is the focus of this study. According to general level, a social distance of 1m was recommended for low-intensity training and 2m for high-intensity training (yellow level). In a closed room, social distance is directly proportional to density of people.
Airborne transmission has been identified as one of the modes of transmission of the SARS COV-2 virus [2]. Therefore, this study carried out field measurements to evaluate the indoor infection risk in the gym where social distancing has been implemented during the pandemic.
Wells Riley is a risk assessment model that is prevalently used in infection risk evaluation for indoor environments where ventilation is considered as the only mechanism to remove viruses [3].
| (1) |
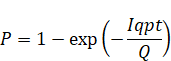
Where, P = infection rate, %; I = number of infected people. p = quanta per hour per person. q = breathing rate m³/h. t = time in hours. Q = ventilation rate m³/h.
Under steady state, the mass balance equation for the quantity of pollutants generation can be expressed:
| (2) |
Where, G = emission rate of CO₂ inside of the room, g/h. cr and ci = concentration measured at the exhaust and supply air of the ventilation system, g/m³.
In this study, measurements were done in two fitness centres, Sit Portalen and Sit Gløshaugen, in Trondheim, to measure the ventilation rate in rooms with different activities and determine the infection risk. In Portalen the measurements were done in a larger room, where Yoga was performed, while in Gløshaugen, the measurements took place in a smaller room, where Tabata was performed.
The measuring procedure was done with respect to the participants in the group activities. In both rooms, the instruments were placed in a corner, in front of the participants (facing the instruments) with a 2-3 m distance from the walls and the people to minimize the impact.
For results:
· Measurements taken every 15 minutes in an hour
· CO₂ concentration, every 15 minutes for 4 minutes in a row
· Last 4 minutes, values of every 20 seconds recorded
For the measurements in both gyms, the following instruments were used: Thermal anemometer, Elma DT – 802.
Activity | Number of people performing the activity | Number of people NOT performing the activity | Volume of the room [m³] |
Yoga (Portalen) | 15 | 2 | 445.72 |
Tabata (Gløshaugen) | 13 | 2 | 286.68 |
Figure 1 shows the change of CO₂ concentration in the two gyms. The measurements started at 0mins, when people came into the room, and the class ended at 55 minutes. The CO₂ concentration in Yoga room is 2500-2700 ppm, and there is a slow rise over time. It falls back to the initial level 5 minutes after the end of the course. The CO₂ concentration in Tabata room is around 700-1000 ppm. A slight increase can be observed during the whole time. The values obtained by steady state methods is used as the calculation values. Ventilation in the two rooms is 2063.9 m³/h, in Tabata room (7.2 ACH), and 343.2 m³/h in Yoga room (0.76 ACH).
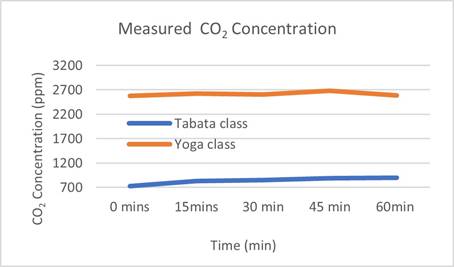
Figure 1. Measured CO₂ concentration in two rooms.
Based on the literature [4], the virus release rate of Yoga activity was set at 5.6 quanta/h·person and for Tabata activity at 13.5 quanta/h·person. The respiration rate in Yoga room was 1.38 m³/h, and in Tabata room was 3.3 m³/h [5].
Assuming, usable area of the room to be 80% of total area, the per capita area can be obtained according to the number of people. By maintenance of distance between people, the relationship of the number of infected people to social distance can be obtained.
Figures 2 and 3 show the variation of the number of infections with social distance in the two rooms, with various sources of virus infection. The estimated number of infections was calculated using the Wells Riley Model. In Tabata class according to Wells Riley model, when there was only one source of release, the infection rate for an hour was 2.14%. With social distance of 1m, the room can hold a maximum of 88 people. Calculating, the number of infected people in the whole room 1.88, 3.72 and 5.52 respectively at the source of one, two and three people. Considering 2m social distance, the maximum number of people in the room is 22. Accordingly, the number of infected people dropped to 1.28, 0.93 and 0.47, These values decrease to 0.21, 0.42 and 0.64 with social distance of 3 meters (The maximum number pf is 11).
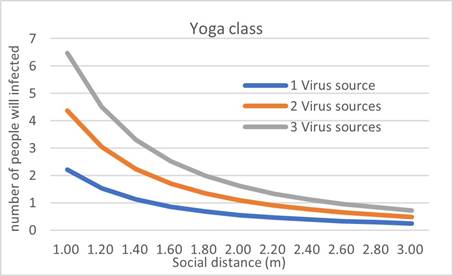
Figure 2. The relation between the number of people likely to get infected and the distance between the participants in Yoga class. This relation is shown for different numbers of infected people in the room/virus sources.
In Yoga class, probability with presence of one infected was 2.23%. When the social distance is 1 m, maximum number of people in the room is 99, and the expected number of infected people after a class is 2.2, 4.36 and 6.46 respectively when the virus sources are 1, 2 and 3. These value decease dramatically to 0.24, 0.48 and 0.71.
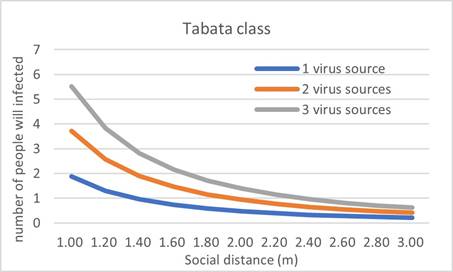
Figure 3. The relation between the number of people likely to get infected and the distance between the participants in Tabata class. This relation is shown for different numbers of infected people in the room/virus sources.
Yoga and Tabata
The measurements for CO₂ in Yoga room were higher than the Tabata room (no interval between classes) and it was around 2500-2700 ppm. This combined with a low ventilation rate and a very heavy breathing of the participants throughout the exercises caused high CO₂ levels. Activities started with subtle exercises, increased in the middle, and again relaxed towards the end, as it is shown in Figure 1.
In Tabata, activities started slowly then increased and remained mostly constant in a high level, except the last minutes that included lighter activities. Figure 1 shows that the CO₂ concentration increased throughout the whole class. The graph corresponds well with the activity level, except at the end where concentration was expected to decrease. This increase is due to opening of the door at the end of the class and the CO₂ concentration that was higher outside the room.
Social Distancing
In Yoga room, with a social distance of 1m, maximum number of infections is 2.2, is high. However, when the number is limited to less than 20, it drops below 0.5. When the ventilation rate increased, this value decreased further. Therefore, it is not enough to limit social distancing to reduce the possibility of infection, especially when ventilation airflow rate is low. Considering ventilation volume, room type and ventilation method, it is important to effectively reduce infection by using multi measures like social distancing and increased ventilation rate. Related results were found in Tabata room. However, the ventilation rate was high, so the only possibility to reduce the infection risk is to reduce the number of participants. At the time of this study, the number of people in the room was 13, and then the expected number of infections was 0.32 when one person released the virus.
Figures 2 and 3 show that the social distance requirement has a profound influence on the infection risk. Even though this analysis does not consider direct exposure via droplet transmission, the results have shown that social distance also affects the risk of airborne infection.
As mentioned, the requirements distinguish between the social distance for low and high intensity activity. Yoga room has less ventilation than Tabata room, but their infection rates are almost similar. Because, in Yoga room people had a lower activity level but had many breathing exercises. If the rooms were similar with same ventilation conditions, the airborne infection risk in Yoga room would have been smaller than the risk in the Tabata room, with the same social distancing. The distance dependent on activity level can be assumed to be a more important infection risk for the droplet transmission than the airborne transmission.
The infection risk was calculated and discussed in relation to the Norwegian requirements on social distancing. Social distance alone is not sufficient to eliminate the airborne infection risk during COVID-19 pandemic. Combined measures, for example social distancing with an appropriate ventilation rate to create a safer indoor environment should be considered. As observed, in Yoga room the ventilation rate was low, and this had a larger influence on infection risk than social distance had. Considering different activity levels, room volume and ventilation type are quite important to reduce the infection risk.
The categorization of the rooms, in high and low activity levels, is quite reasonable as the CO₂ emitted from people during the exercise works as an indicator for the infection risk. Therefore, the results of this study suggest that infection control measures should be classified according to the activity level in different built environments with different ventilation flow rate. It also indicates that if it is not feasible to change the ventilation flow rate, then enlarging social distancing requirements may help to reduce the infection risk to a similar level.
[1] COVID-19 — Infection control measures for fitness centres — Rev.4. 2021, Standard Norge.
[2] Li, Y., et al., Probable airborne transmission of SARS-CoV-2 in a poorly ventilated restaurant. Building and Environment, 2021. 196: p. 107788.
[3] Sze To, G.N. and C.Y.H. Chao, Review and comparison between the Wells–Riley and dose-response approaches to risk assessment of infectious respiratory diseases. Indoor Air, 2010. 20(1): p. 2-16.
[4] Buonanno, G., L. Stabile, and L. Morawska, Estimation of airborne viral emission: Quanta emission rate of SARS-CoV-2 for infection risk assessment. Environment International, 2020. 141: p. 105794.
[5] Kurnitski, J., Ventilation rate and room size effects on infection risk of COVID-19. REHVA Journal, 2020. 05: p. 26-31.
Follow us on social media accounts to stay up to date with REHVA actualities
0