

Stay Informed
Follow us on social media accounts to stay up to date with REHVA actualities
|
|
Elizabeth Cooper | Yan Wang |
Dr, LecturerUCL Institute for Environmental Design & Engineering | Dr, Research AssociateUCL Institute for Environmental Design & Engineering |
The premise of the work described here was to determine if a tailored application of building information and communication technologies might improve occupant comfort and health. This work explored the novel concept of connecting the predicted effects of a building control system with a health impact assessment, an important and innovative step in the creation of holistic and responsive building controls.
People in the UK, as with most of the Global North, spend nearly 65% of their time at home, where concentrations of particulate matter less than 2.5 µm in diameter, (PM2.5) can be much higher than in outdoor air due to occupant behaviours such as cooking and smoking. PM2.5 has been linked to many serious health effects, including lung cancer, stroke, heart disease, and asthma. The good news is that previous research has reported that portable home air purifiers (HAPs) equipped with High Efficiency Particulate Air (HEPA) filters can effectively reduce PM2.5 levels in the rooms in which they are used. An important factor which has the potential to conflict with air filtration strategies in buildings, is occupants’ operation of windows. The operation of windows also exerts a substantial impact on thermal comfort and building energy consumption. In this context, the research presented here aimed to develop a novel building control framework in which the operation of windows and the use of portable home air purifiers were optimised for energy efficiency and occupant health.
Building control systems play a central role in building operations and performance. Satisfying occupants’ comfort and minimising building energy consumption and carbon emissions are generally the intentions behind the design of a building control system. These systems, in general, share a common structure; first, the sensor measures an environmental parameter (e.g., temperature, CO₂ concentration); second, the sensor sends collected data to the controller which then uses pre-programmed control logic to determine the direction of change (if any). Window control systems have become a research topic gaining increasing interest in recent years, and research into HAPs has, independently, become a growing area of study. Although both automatic window controls and HAPs have, in recent years, but of increasing interest, an integrated system, which controls both window operations and HAPs, has not yet been investigated.
The proposed control framework included two modes; for the non-heating period, the control framework has both HAP and window controls running in parallel; during the heating period, windows are set to be closed, and the mechanical ventilation with heat recovery (MVHR) system operates continuously to provide background ventilation, and the HAP is enabled. The two control modes are shown schematically in Figures 1 and 2. In both modes, when the indoor PM2.5 concentration reaches the defined ‘HAP-on’ threshold (15 µg/m³) the HAP switches on and continues to operate until the concentration falls below the defined ‘HAP-off’ threshold (5 µg/m³).
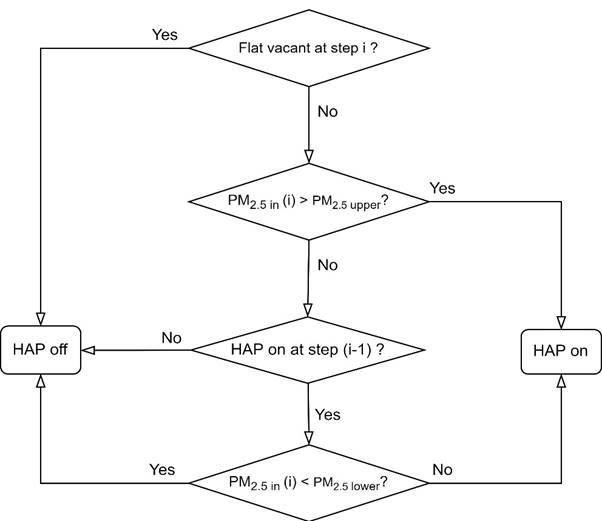
Figure 1. Algorithm for HAP control. (PM2.5 in: indoor PM2.5 concentration, PM2.5 upper: HAP-on threshold, PM2.5 lower: HAP-off threshold, i: time step).

Figure 2. Algorithm for window control. (Tin/Tout: indoor / outdoor temperature, Tcomfort.upper / Tcomfort.lower: upper / lower limit of comfort temperature, PM2.5 in / PM2.5 out: indoor / outdoor PM2.5 concentration, ΔPM2.5: the maximum accepted difference between indoor and outdoor PM2.5 concentration, i: time step).
When the residence is occupied, the default state of the window is fully open to optimise natural ventilation. However, the window is set to fully close when certain conditions are met; either the indoor temperature falls outside the limits of EN 16798-1 Category II adaptive comfort temperature, or when both the outdoor PM2.5 concentration is higher than that indoors, and the indoor temperature is within the comfort zone, to reduce the working load of the HAP.
Quantitative health impact assessments are used to estimate future rates of mortality and morbidity from different interventions compared to what is predicted without such changes. In the work presented here, life-table models were used to quantify the impacts on mortality from reductions in indoor PM2.5-concentrations due to the implementation of the control framework.
The life-table method is based on age- and sex-specific mortality rates, which are used to calculate probabilities of survival by year-of-age and calendar year. An impact assessment is performed using the underlying mortality rates which are adjusted to reflect changes in mortality risk from changes in exposure by applying relative risks calculated using available epidemiological evidence. Individual single-year survival probabilities are multiplied together to calculate cumulative probabilities of survival over multiple years. These cumulative survival probabilities are applied to a population allowing the calculation of life years lived by the population (where one life year is a full year of life lived by one person), which in turn can be used to estimate the average remaining life expectancy per person by age.
The proposed hybrid control framework, along with either HAP or auto-window control alone for comparison, was tested in building simulations for a one-bedroom apartment. The simulation results for a summer week are presented below.
In the baseline scenario, without any control measures, there were morning and evening peaks of indoor PM2.5 concentration, and the daily mean of indoor PM2.5 concentration exceeded the WHO 24-hour limit (15 µg/m³) for most of the week. However, the indoor temperature remained within the comfort range the entire week (Figure 3).
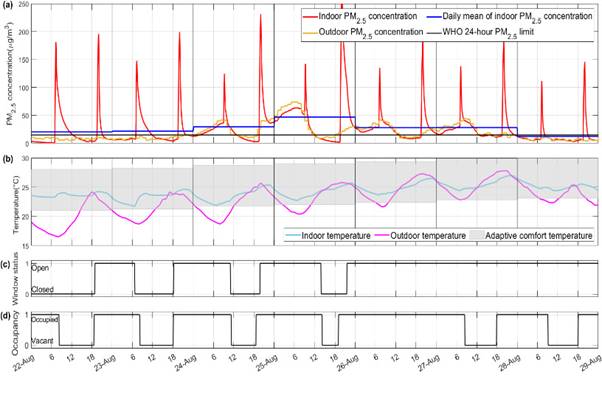
Figure 3. Summer week: Baseline. (a) Indoor and outdoor PM2.5-concentrations with the daily mean of indoor PM2.5 concentration compared with the WHO guideline; (b) indoor, outdoor and adaptive comfort temperatures; (c) window state schedule; (d) occupancy schedule
In the auto-window control mode (Figure 4), there was a significant reduction in the peaks of indoor PM2.5 concentration. The number of days exceeding the WHO limit of PM2.5 concentration fell by two from the baseline and occupant thermal comfort was still satisfied.
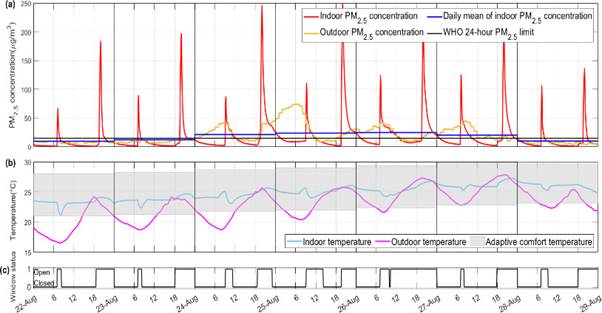
Figure 4. Summer week: Auto-window mode. (a) Indoor and outdoor PM2.5-concentrations with the daily mean of indoor PM2.5 concentration compared with the WHO guideline; (b) indoor, outdoor and adaptive comfort temperatures; (c) window state schedule.
Figure 5 shows the HAP control mode where the peaks of indoor PM2.5-concentrations were further reduced from both baseline and auto-window control. However, because of high outdoor PM2.5 levels, even with the use of HAPs there were still two days when the daily mean concentration of indoor PM2.5 was above the WHO limit.
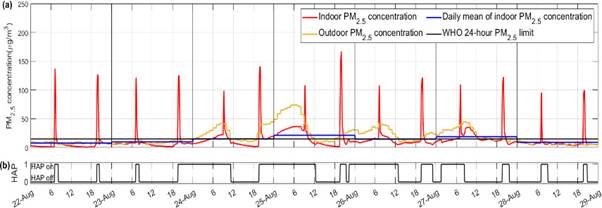
Figure 5. Summer week: HAP mode. (a) Indoor and outdoor PM2.5-concentrations with the daily mean of indoor PM2.5 concentration compared with the WHO guideline; (b) HAP operation schedule.
The hybrid control mode, shown in Figure 6, represents the proposed control method. With both HAPs and windows controlled, the indoor PM2.5 concentration never decreased exceeded the WHO daily limit, whilst indoor temperature was maintained within the comfort range.
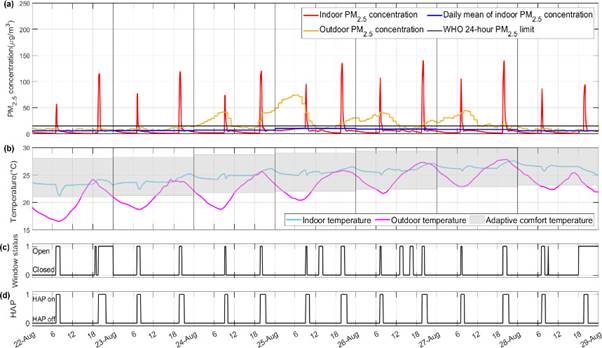
Figure 6. Summer week: Hybrid mode. (a) Indoor and outdoor PM2.5-concentrations with the daily mean of indoor PM2.5 concentration compared with the WHO guideline; (b) indoor, outdoor and adaptive comfort temperatures; (c) window state schedule; (d) HAP operation schedule.
The major advantage of the joint control of HAPs and windows was that the window could be shut when outdoor pollution was high before an accumulation of PM2.5 could occur indoors. In this way, the indoor PM2.5 concentration was lowered while optimising the HAP operation and efficiency. Meanwhile, the control algorithm was directed, when the outdoor air quality was good, to open the window to allow for natural ventilation.
The simulated reductions in indoor PM2.5-concentrations, from baseline, for each of the control modes were used to estimate the mean years of life gained (YLGs) for females and males in the UK over a lifetime (97 years). The mean YLGs for males were approximately 6.5 million, 15 million, and 18 million for the automatic window/MVHR, HAP, and hybrid modes respectively. For females YLGs were approximately 6 million, 14 million, and 16 million for the three intervention scenarios, respectively (Table 1). The reduction in exposure to PM2.5 from the implementation of the hybrid mode added a mean of nearly 6 months of life for both males and females.
Table 1. Summary of life-table model estimates of changes in mortality from different environmental control strategies based on modelled PM2.5-concentrations in case study flat.
Males | Females | |||
Control mode | YLG Mean | Mean days gained | YLG Mean | Mean days gained |
Auto-window/MVHR | 6,557,926 | 73 | 5,948,462 | 64 |
HAP | 15,209,453 | 168 | 13,739,074 | 148 |
Hybrid | 17,940,660 | 199 | 16,188,821 | 175 |
For building designers and engineers, this work highlights the importance of recognising health impacts, as well as energy efficiency and environmental impacts, related to occupant-centric building design and operation.
For policymakers, this research adds technical evidence of the impact of including health metrics in the building sector.
The implementation of smart building control systems, such as those modelled here, has the potential to reduce exposure to indoor pollutants such as PM2.5 which could have substantial population health benefits.
Follow us on social media accounts to stay up to date with REHVA actualities
0